Anaesthesia and sedation
After proper positioning, a local anaesthetic is administered to numb the specific area to be treated. This local anaesthetic helps to minimise any pain or discomfort during the procedure. In some cases, conscious sedation may also be used to help you relax and feel more comfortable.
Needle insertion
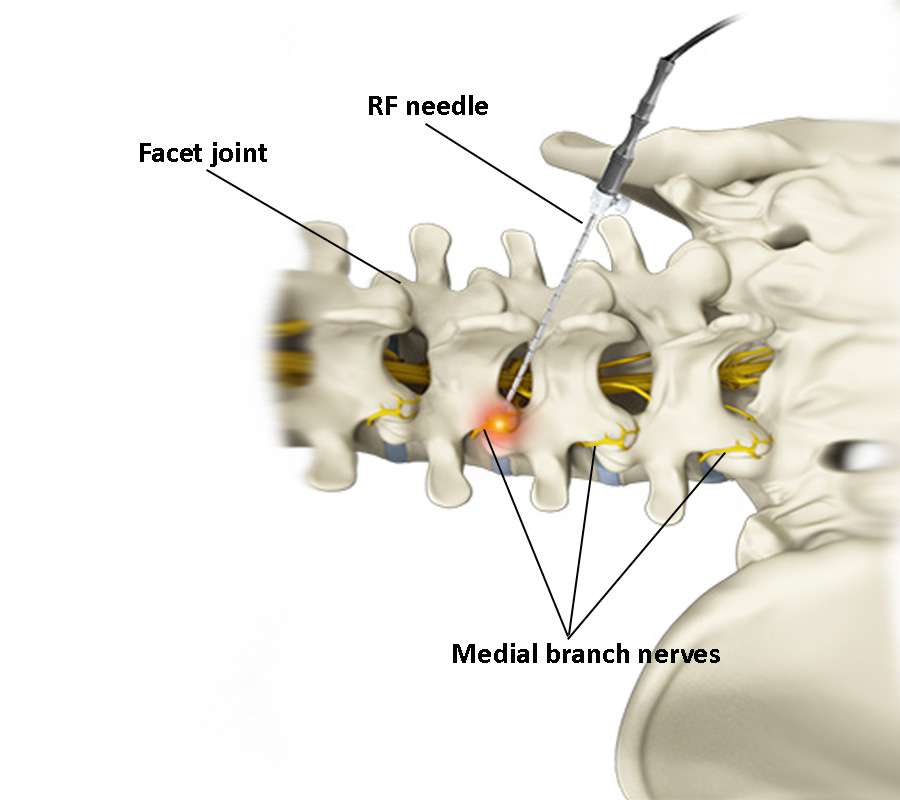
After the anaesthetic and sedation have taken effect, a small, specialised RF needle is carefully guided to the medial branch nerve under fluoroscopic guidance. The aim is to place the needle close to the nerve while avoiding vital structures. After the needle is placed in the right place fluoroscopically, motor and sensory stimuli are given. Small adjustments can be made to be in the closest position to the medial branch nerve.
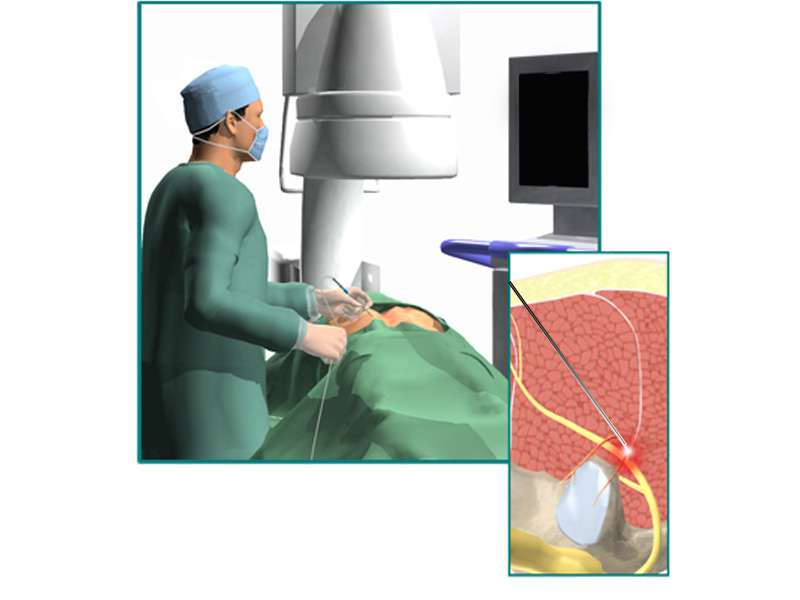
Radiofrequency ablation (denervation or thermocoagulation)
Once the needle is in the correct position, the radiofrequency (RF) ablation procedure begins. RF generates high-frequency electrical currents that heat the tip of the needle. This heat is delivered precisely to the nerve, causing it to coagulate, or essentially ‘burn’, and disrupting its ability to transmit pain signals. The temperatures used are carefully controlled to avoid excessive damage to surrounding tissue.
Post-procedure observation
After the RF thermocoagulation procedure, you will be kept under observation for a short time to monitor your immediate post-procedure condition. This is to ensure that there are no complications and that your vital signs are stable. It’s common for patients to experience mild discomfort or soreness at the treatment site during this time.
Recovery after the procedure
You’ll usually spend a short time in a recovery room where the effects of sedation or anaesthesia wear off. Your healthcare provider will give you post-operative care instructions, which may include recommendations for rest, over-the-counter pain relief, and any activity restrictions. It’s important to follow these instructions to ensure a smooth recovery.
Potential complications of medial branch nerve radiofrequency ablation
Complications associated with medial branch nerve RF ablation are rare, but they can occur. The following are some of the potential complications that can occur with this procedure:
Infection: Infection is a risk common to all invasive procedures, including medial branch nerve denervation.
Bleeding: Bleeding is a rare complication, but is more common in patients with underlying bleeding disorders.
Allergic reaction: A potential allergy is usually to the X-ray contrast agent and rarely to the local anaesthetic.
Aggravation of pain symptoms: In rare cases, patients may experience an increase in pain symptoms after the procedure.
Discomfort at the injection site: Patients may experience some discomfort or soreness at the injection site, but this usually resolves within a few days.
Nerve or spinal cord damage or paralysis: Although very rare, damage can occur as a result of direct trauma from the needle, or secondarily from infection, bleeding causing compression, or injection into an artery causing blockage.
Follow-up and pain relief assessment
In the days and weeks following your procedure, you’ll have a follow-up appointment with your physician. During this visit, your pain relief will be assessed and any necessary adjustments or additional treatments may be discussed.
Keep in mind that the specific details of each procedure may vary depending on the healthcare facility, the healthcare provider’s practices, and individual patient needs. Always consult with your healthcare provider for personalised information and guidance regarding medial branch RF denervation.